This is a perfect example of the stunt that you pull in this forum over and over again. Now, just a few days ago, you and I discussed the myth that Humes only learned of the throat wound on the morning after the autopsy. I presented you with evidence that debunks this myth. I cited the fact that we know from the ARRB materials that the throat wound was probed. I cited the fact that a good friend of Humes's, Jim Snyder of CBS's DC bureau, confidentially informed CBS producer Robert Richter that Humes told him that he was aware of the throat wound during the autopsy (we learned this when Richter's 1/10/67 internal memo to CBS producer Les Midgley later surfaced).
You're citing two layers of hearsay by non-medical people of a "conversation" not recorded?
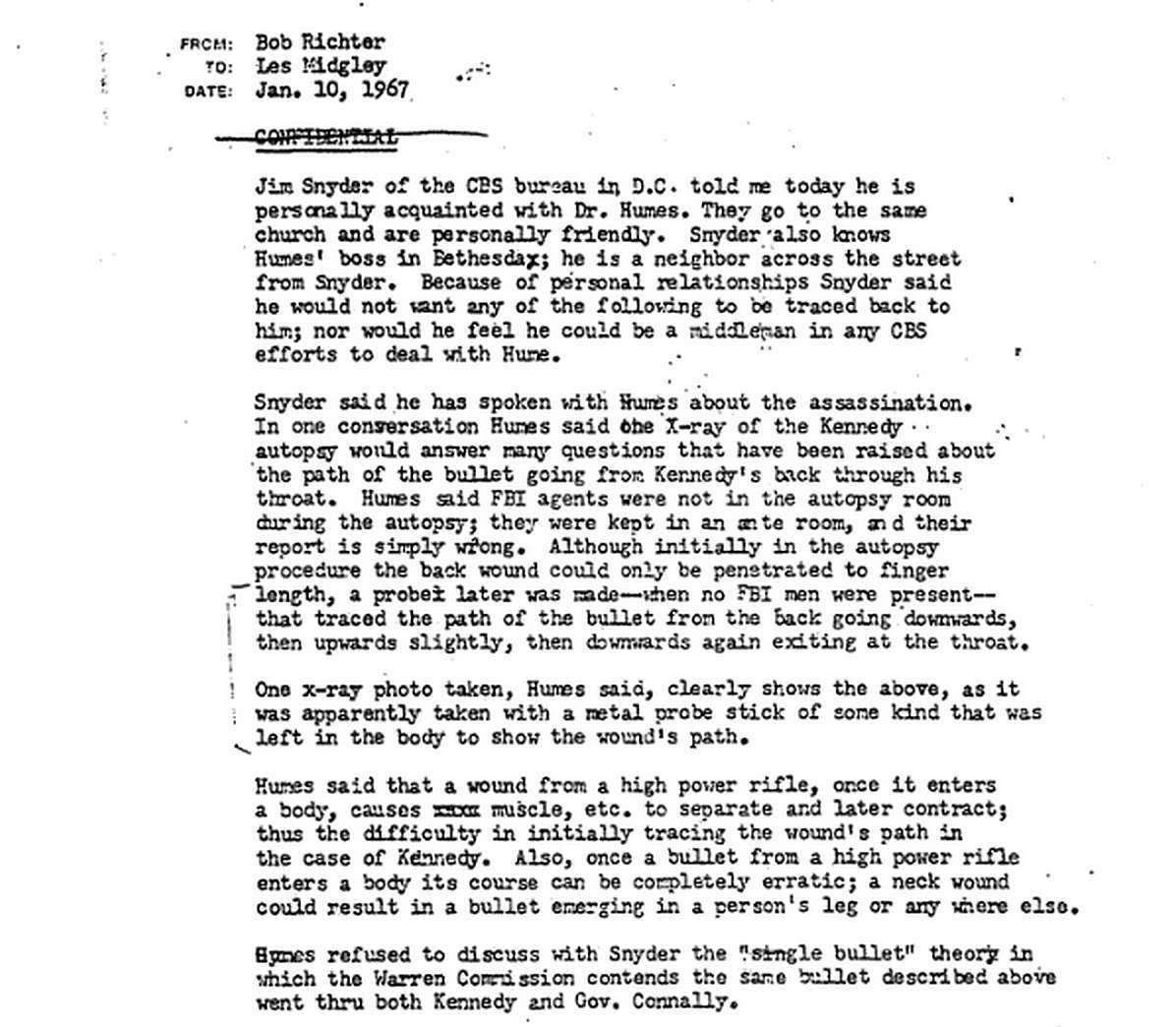
Isn't CBS part of the Mass Media Coverup? What x-ray with a probe did the three pathologists describe in their 1967 "Military Review" or in sworn testimony? Why does Humes seem to probe the whole neck transit, then say he doesn't want to use it to authenticate the SBT?
I cited the fact that we now know that the first two drafts of the autopsy report said nothing about a bullet exiting the throat (you keep ignoring the fact that there were two drafts, not just one).
Is there some law that pathologists can only write a set number of drafts?
And I cited the fact that James Jenkins, one of the medical technicians at the autopsy, witnessed the probing of the back wound and could see that the wound did not enter the lining of the chest cavity, that he could see the end of the probe pushing against the chest cavity's lining.
You wrote:
"And we also now know that Jenkins told the HSCA that the back-wound
enabled Humes "to reach the end of the wound" and that the wound tract
was "not into the chest cavity.""
Not the same as the probe pushing against the cavity lining.
Yet, here you are, in a different thread, once again repeating the myth that Humes knew nothing about the throat wound during the autopsy, and you're doing this while saying nothing about the contrary evidence that I myself presented to you just a few days ago.
I should add that I did not even present all the evidence that debunks the myth. Here is some additional evidence that refutes it:
* Amazingly, and perhaps in a back-handed effort to reveal that the autopsy doctors knew about the throat wound during the autopsy, Dr. Boswell told the ARRB that after the back wound was probed following the removal of the chest organs, the probing revealed that the wound track exited the throat wound, that the probe actually came out from the throat wound!
Now, of course, his claim about the throat wound being identified as the exit wound via probing was contradicted by several autopsy witnesses, not to mention that it contradicts the story that Boswell, Finck, and Humes told for years about when they learned of the throat wound.
Autopsy photographer John Stringer (who was also the director of medical photography at the Naval Medical School in 1963) specifically said that the probe did not come out through the neck, and Sibert and O'Neill emphatically said that at the end of the autopsy the autopsy doctors had no doubt whatsoever that the back wound had no exit and that the bullet found in Dallas had worked its way out of the back wound during cardiac massage.
When asked about the Sibert and O'Neill report, Boswell falsely claimed that Sibert and O'Neill weren't in the autopsy room when the back wound was probed after the chest organs were removed. Actually, Sibert and O'Neill saw the initial probing and saw the probing that was done with the chest organs removed, and they remained at the autopsy until the body was prepared for burial. Sibert left the autopsy room for short periods, but O'Neill remained in the room "through the time that the autopsy was completed," and he saw the autopsy doctors remove their gloves and call for the morticians to prepare the body for burial.
* Stringer told the ARRB that a probe was inserted into the throat wound, and he added that he believed the body was propped up so the torso was in a vertical position when the probe was put into the throat wound.
* Dr. John Ebersole, the autopsy radiologist, told the HSCA that Humes was aware of the throat wound during the autopsy.
* Dr. George Burkley, JFK's personal physician, knew about the throat wound because he was in the ER at Parkland Hospital helping the Parkland doctors treat JFK. He supplied the Parkland doctors with hydrocortisone because of JFK's adrenal condition: "Burkley produced three 100-mg vials of Solu-Cortef from his bag, murmuring, 'Either intravenously or intramuscularly'" (William Manchester, The Death of a President, Harper & Row, New York: 1967, p. 184). Burkley arrived in the ER before Dr. Perry arrived, and Dr. Perry was the one who did the tracheostomy over the throat wound, so Burkley surely saw the throat wound, just as did the other doctors and nurses who were in the room before Dr. Perry arrived. And, of course, Dr. Burkley was also at the autopsy and spoke with the autopsy doctors during the autopsy.
* Nurse Audrey Bell, the Supervising Nurse of Operations and Recovery at Parkland Hospital, revealed in 1997 that Dr. Perry complained to her on the morning after the autopsy that he had gotten almost no sleep the night before because unnamed persons at Bethesda Naval Hospital had been pressuring him on the telephone all night long to change his opinion about the throat wound, and to describe it as an exit wound rather than an entrance wound.
* Dr. Perry and other Parkland doctors held a televised press conference barely an hour after JFK died, about six hours before the autopsy began, and Dr. Perry stated three times during the press conference that JFK's throat wound was an entrance wound.
The story that the autopsy doctors didn't know about the throat wound until the morning after the autopsy was invented to explain Humes's destruction of the first two versions of the autopsy report. A story had to be concocted that would at least appear to excuse Humes's highly unusual and illegal action of destroying autopsy drafts. Again, we now know that the first two drafts said nothing about a bullet exiting JFK's throat.
By the way, Dr. Robert Canada, a high-ranking Navy medical officer at the autopsy, said that the back wound was at around the level of T3 and that the bullet "did not exit." At the time of the autopsy, Dr. Canada was a Navy captain and was the director of the Naval Medical School at Bethesda Naval Hospital. Dr. Canada also said that there was a large "avulsed" (blown out) wound in "the right rear of the president's head." Dr. Canada shared this information in a 1968 interview with Dr. Michael Kurtz, a historian at Southeastern Louisiana University. Dr. Canada asked that Dr. Kurtz not publish his comments until 25 years after his death, and Dr. Kurtz honored that request.
To be specific, Humes claimed he saw bruising on top of the pleural dome, which is above the top of the right lung. However, no autopsy photos show this damage, even though Humes repeatedly claimed that photos were taken of it. Furthermore, Jenkins said he saw no bruising on the top of the pleural dome but that he did see bruising at the of the right lung's middle lobe.
Since you're citing Jenkins, he said the autopsy doctors had no knowledge of the throat wound during the autopsy. The Silbert-O'Neill Report also says as much.
What Finck told the ARRB about the extent of the probing:
Q: When you were performing the autopsy of President Kennedy,
did you make any attempts to track the course of the bullet
A: Yes.
Q:that you referred to as the upper back?
A: Yes. That was unsuccessful with a probe from what I remember.
Q: What kind of probe did you use?
A: I don't remember.
Q: Is there a standard type of probe that is used in autopsies?
A: A non-metallic probe.
Q: In using the probe, did you attempt to determine the angle of the
entrance of the bullet into President Kennedy's body?
A: Yes. It was unsuccessful from what I remember.
Q: In the probes that you did make, did you find any evidence that
would support a bullet going into the upper back and existing from the
place where the tracheotomy incision had been performed?
A: From what I recall, we stated the probing was unsuccessful.
...
Q: Do you have any recollection of photographs being taken with probes
inserted into the wounds?
A: I don't.
...
Q: At the time you concluded the autopsy, on the night of November
22nd-23rd, did you have any conclusion in your own mind about what
had happened to the bullet that entered the upper thoracic cavity?
A: No. And that was the reason for the phone call of Dr. Humes the
following morning, and he found out there was a wound of exit in the
front of the neck. But at the time of the autopsy, we were not aware
of that exit wound in the front of the neck.
...
Q: Sure. Did the angle of the probe when you inserted the probe into
the wound, begin in a direction that pointed down into the thoracic
cavity rather than out the throat?
A: I don't think I can answer the question, because we said the probing
was unsuccessful. So how can I determine an angle if the probing
was unsuccessful?
_____
Humes to the ARRB:
A. My problem is, very simply stated, we had an entrance wound high
in the posterior back above the scapula. We didn't know where the
exit wound was at that point. I'd be the first one to admit it. We knew
in general in the past that we should have been more prescient than
we were, I must confess, because when we removed the breast plate
and examined the thoracic cavity, we saw a contusion on the upper
lobe of the lung. There was no defect in the pleura anyplace. So it's
obvious that the missile had gone over that top of the lung.
...
... it's helpful to take a long probe and put it in the position. It can tell
you a lot of things. If you know where the point of entrance and the
point of exit are, it's duck soup. But for me to start probing around in
this man's neck, all I would make was false passages. There wouldn't
be any track that I could put a probe through or anything of that nature.
It just doesn't work that way.
Q. Was any probe used at all to track the path
A. I don't recall that there was. There might have been some abortive
efforts superficially in the back of the neck, but no.
...
Q. Do you recall any photograph or X-ray that was taken with a probe
inserted into the post thorax?
A. No, absolutely not. I do not have a recollection of such.
_____
Boswell to the ARRB:
Q. Previously in the deposition, you've made reference to there being a
probe to help track the direction of the neck wound. Do you recall that?
A. Mm-hmm.
Q. Could you tell me about how long the probe was or describe the
dimensions of the probe?
A. It's a little soft metal instrument that looks like a needle with a blunt
end on one end and a flattened end on the other, like a needle that you
would knit with or something. And it's, I would say, eight inches long,
blunt on one end and sort of has a sharp point on the other end.
Q. Were there any X-rays taken with the probe inside the body that
you recall?
A. No.
Q. How far in did the probe go?
A. Very short distance. Three inches, about.
Q. Were there any photographs taken with the probe inserted?
A. I doubt it.
...
... When we saw the clothing, we realized that where I had drawn this was
if you looked at the back of the coat, it was in the exact same place. But the
coat had beenwas up like this. He was waving, and this was all scrunched
up like this. And the bullet went through the coat way below where this
would be on his body, because it was really at the base of his neck. And the
way I know this best is my memory of the fact thatsee, we probed this hole
which was in his neck with all sorts of probes and everything, and it was such
a small hole, basically, and the muscles were so big and strong and had
closed the hole and you couldn't get a finger or a probe through it. But when
we opened the chest and we got atthe lung extends up under the clavicle
and high just beneath the neck here, and the bullet had not pierced through
into the lung cavity but had caused hemorrhage just outside the pleura.
And so if I can move this up to hereit's shown better on the front, actually.
The wound came through and downward just above the thoracic cavity and
out at about the thyroid cartilage. So if you put a probe in this and got it back
through like this, that would come out right at the base of the neck.


